






Sign up for the QMED & MD+DI Daily newsletter.
Building Quality into Device Clinical Trials
Marcarelli
+3
19 Min Read
.svg?width=850&auto=webp&quality=95&format=jpg&disable=upscale "Building Quality into Device Clinical Trials")
Many warning letters issued by CDRH cite violations of good clinical practices found during bioresearch monitoring (BIMO) inspections. Tables I–III detail the types of violations that are often cited, including operations of sponsors, clinical investigators, and institutional review boards (IRBs; see also Figures 1–2). Such violations not only lead to risks to public health but also result in delays in getting products to market because of inaccurate or unusable data.
|
Serge |
FDA's Division of Bioresearch Monitoring at CDRH (also referred to as BIMO) has studied the quality of device research over the past two years. The agency has also observed best practices during that review. FDA looked at the quality of device research in terms of its fitness for use in meeting reasonable safety and effectiveness criteria and in ensuring the ethical oversight of human research subjects.1
|
Toth-Allen |
It is essential that FDA support innovation and encourage sponsors to develop effective approaches to gain greater control over device research. To speed products to market and improve the bottom line, sponsors should conduct high-quality and ethical clinical research. This article discusses how to better ensure human-subject protection and how to strengthen the sponsor-IRB relationship. Future articles will cover how to conduct device clinical research and how to adapt already existing manufacturing quality systems, such as the CAPA system, for use in medical device clinical research.
FDA Inspection Goals
|
Harris |
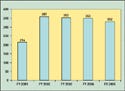
In FY 2006 and FY 2007, FDA plans to conduct 300 domestic and 10 foreign medical device BIMO inspections. In FY 2005, FDA exceeded its goal of 280 domestic and 15 foreign BIMO inspections by conducting 332 such inspections.2,3
|
Immel |
FDA's approach to BIMO inspections has traditionally focused on data audits of premarket approval (PMA) applications. Although this approach has enabled FDA to validate the data submitted in marketing applications, inspections performed after the research was complete have had little effect on ongoing clinical trials. Beginning in FY 2004, FDA began assigning inspections earlier in the process, during the investigational device exemption (IDE) phase. FDA believes that this has enabled it to identify systemic problems and protect exploitable or vulnerable populations. The focus of these inspections is informed consent, IRB review and approval, protocol adherence, device accountability, adverse-event reporting, data monitoring, and data collection, rather than simply data verification.3
CDRH currently has about 1000 active IDEs for high-risk investigational devices (such as artificial hearts and drug-eluting stents).3 FDA is interested in expanding its presence with regulated industry by using a risk-based site-selection strategy for its inspections. This strategy places more emphasis on the following areas:
• Detection of scientific misconduct.
• Data auditing and validation to support the device review process.
• Innovative devices with greater potential for affecting public health.
• Vulnerable populations, such as the elderly, pediatric patients, and minorities.
Human-Subject Protection
Strengthening the Sponsor-IRB Relationship. Sponsors and clinical investigators should be aware of FDA's requirements for the function and operation of IRBs. That information is contained in 20 CFR 56.1,4 A better understanding may help improve interactions among sponsors, clinical investigators, and IRBs. FDA's guidance document, “Sponsor-Investigator-IRB Interrelationship,” addresses this topic.5 The sponsor-IRB relationship is often the least understood link of the research network.
Human-subject protection is not just an IRB function. All three entities—the sponsor, the IRB, and the clinical investigator—have a reciprocal relationship. They share a common interest in human-subject protections and data integrity, and they should be communicating during the entire lifetime of the trial. FDA's regulations set out reporting requirements so that each entity is notified of important events that occur during the study to help ensure protection of the rights and welfare of human research subjects.1
Although FDA regulations do not prohibit direct sponsor-IRB contact, most sponsor-IRB interaction occurs through the investigator who conducts the clinical study. The sponsor and investigator agree to this interaction when they sign an Investigator's Agreement. FDA encourages sponsors to develop Investigator's Agreements that discuss this interaction in detail.
|
Table I. (click to enlarge) Sponsor deficiencies, FDA Bioresearch Monitoring medical device inspectional findings, FY 1998–2005. Percentages shown are total BIMO device inspections in which that particular problem was found during the year. |
IRB Approval before Study Begins. One of the sponsor's responsibilities under 21 CFR 812, “Investigational Device Exemptions,” is that the sponsor must ensure that IRB approval is obtained before a clinical study begins at a particular site.6 Yet in 2004, CDRH found during its BIMO inspections that 11% of medical device studies started before IRB approval was received. In 2005, the agency found that failure to obtain IRB approval before the study was started continued to be one of the top five areas of investigator noncompliance (see Table I).1
To avoid such problems, FDA encourages sponsors to develop effective approaches to ensure that device studies are not started until after IRB approval is received. Sponsors must also ensure that all reviewing IRBs are promptly informed of significant new information. This information includes any changes to the protocol or to the device that would affect subjects' willingness to continue participating in the study. In addition to documenting a sponsor's interactions with the IRB, a sponsor must retain all correspondence with the IRB. Sponsors can use this correspondence as a human-subject protection measure. It can ensure that the required reporting to the IRB has occurred and that the initial and continuing IRB review has been obtained. Sponsors should retain files that document their interaction with the IRB.1
|
Table II. (click to enlarge) Investigator deficiencies, FDA Bioresearch Monitoring medical device inspectional findings, FY 1998–2005. IC = informed consent. |
Records and Reports. Sponsors are also expected to keep records of the names and addresses of the IRBs they use. They must also report any problems with a device—or any unanticipated adverse events that occur during the trial—to the IRBs. Sponsors must notify all IRBs of any IRB or FDA withdrawal of a device study. IRBs use this information to ensure that the research volunteers at their institution are properly notified and treated as appropriate.
Sponsors must notify IRBs within 30 working days when an investigator has been asked to return, repair, or otherwise dispose of a device. IRBs want to follow up with the clinical investigators at their institution to learn whether any other devices have had similar problems. Sponsors are required to notify IRBs about any device problems, such as device failures, damaged devices, or sterility problems. In short, anything that relates to the safety of human subjects must be reported to the IRB. This is true even if a device malfunctions. Even if sponsors believe that a malfunction had no effect on patient safety, they still must report any malfunction to the IRB, because it may affect the patient's willingness to continue the study or human-subject protection.
Sponsors must also provide IRBs with progress reports at least once a year. Some IRBs complain that they don't receive progress reports, and some don't know what to do with them when they get them. They should use the information to help determine the overall status of the study. Sponsors should encourage IRBs to read these reports and to maintain them.
In addition to annual progress reports, sponsors must also provide a final study report to the IRB. This is due six months after the study's conclusion at all sites. Information exchange is part of the shared responsibilities for human-subject protection, and it should be reciprocal.
|
Table III. (click to enlarge) IRB deficiencies, FDA Bioresearch Monitoring medical device inspectional findings, FY 1998–2005. SR = significant risk device; NSR = nonsignificant risk device. |
IRB Responsibilities. IRB responsibilities are described in 21 CFR Part 56.4 FDA will cite IRBs for any deficiencies in meeting these requirements. FDA currently inspects IRBs about once every five years. In 2005, of the 30 IRBs inspected by FDA, three received FDA warning letters, and two of these three IRBs had received warning letters from their previous inspection. Some IRBs are small, with only 30 or so open research protocols. Others may be very large, with more than 1000 open research protocols. All IRBs, regardless of their size, must fulfill the requirements of 21 CFR 56 if they review and approve FDA-regulated research.
IRBs have considerable latitude in establishing operational procedures. Some IRBs meet weekly; others meet monthly. This can make the management of clinical trials a challenge. Sponsors should become familiar with each IRB's procedures, because not all clinical sites will begin the study at the same time, and protocol amendments will be approved by different IRBs at different times.
When developing procedures, IRBs may wish to review recent FDA warning letter citations to clinical investigators and IRBs. The citations can help IRBs develop forms or questions to ask to prevent similar violations from occurring. Asking investigators such questions can accomplish two things. First, it helps the IRB gather information. Second, it reminds investigators of their research responsibilities.
IRB Initial Review of Device Studies. There are several documents that are normally reviewed by an IRB when determining whether to give approval for a study. These documents should give an IRB sufficient information to determine the risk-benefit ratio of the device study and to determine whether the study should be conducted at its institution. IRBs may require more information, such as patient diaries or patient educational material. FDA regulations and guidance require IRBs to review the following documents:
• Protocol.
• Informed-consent form.
• Device description.
• Results of previous research (preclinical and clinical).
• Advertisements.
• IRB-required forms.
IRBs usually ask standard initial questions on the IRB-required forms. For example, they will ask for the IDE number, a copy of FDA's approval letter, the clinical investigator's name, and the names of all subinvestigators who may join the study. They will also ask how long the study will last, whether other hospital departments are involved, whether all other hospital department clearances have been received, and the number of subjects expected at that site. These questions are asked to ensure human-subject protection and data integrity in the studies.
Consenting Process. In addition, IRBs should ask the following questions to ensure a proper informed-consent process:
• Who will solicit patients' voluntary consent?
• How will soliciting subjects be handled? Will family members be present?
• Will the environment be void of distractions or interruptions?
IRBs can ask clinical investigators about the process they plan to use to solicit subjects, and sponsors should ask investigators about their consenting processes as well.
Device-Specific Questions. IRBs should also ask clinical investigators the following questions:
• Who will perform the implant or use the device?
• Where will the investigational device be stored?
• Who will have access to investigational devices on the research team?
• What training has the research team received?
• Will there be a field clinical engineer present? If so, are the field clinical engineer's duties described in the protocol? Or are they in the informed-consent document?
|
Figure 1. (click to enlarge) CDRH BIMO inspections, FY 2001–2005. |
Field clinical engineers are typically employees of the sponsor and are often assigned to clinical studies. Duties should not include research activities, such as completing case report forms (CRFs) or monitoring patients. IRBs should ask about field clinical engineers. In one case, when BIMO inspected a clinical investigator site, it found that a field clinical engineer who was supposed to program a pacemaker at the time of implant actually programmed the device throughout the clinical trial and at all the follow-up visits. The protocol had called for the institute's cardioelectrophysiologist to do any follow-up programming. The engineer also performed ECGs, read ECGs, and programmed the pacemakers. He also completed the CRFs and monitored the study for the sponsor.
|
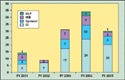
Figure 2. (click to enlarge) CDRH BIMO warning letters issued during FY 2001–2005. CI = clinical investigator. |
If there are to be field clinical engineers, the protocol and the informed consent should describe their assigned duties. IRBs should know their proposed duties, and they should ensure that each engineer is qualified through training and experience to perform the assigned duties. IRBs should also ensure that the duties do not include research activities.
IRB Continuing Review of Device Studies. IRBs should perform a continuing review of each research study at least once a year. Board members need to review the protocol, the current informed-consent form, and IRB-required forms. IRB forms should include questions for the clinical investigator that will help integrate quality into the device clinical trial. IRBs should ask device-specific questions during both initial and continuing review of the research.
Device-Specific Questions. For device studies, IRBs should ask research-specific questions. These could include
• What were the device failures? Include the total number and a description of each.
• Who is implanting the device or using the device?
• Did all subjects meet eligibility (inclusion and exclusion) criteria?
• What are the results of the monitoring visits?
• Was the protocol followed?
• Which subjects received the device?
• How many devices were used, were returned, or were lost (device accountability)?
• Did any subject receive more than one device?
• Have the physicians been successful in implanting the device? Describe any difficulties in implanting the device.
Recently, IRBs have begun to ask for copies of site visit or monitoring reports. Clinical investigators who do not fare well during sponsors' site-monitoring visits may require additional training in the regulations or in protocol requirements. Any retraining should be documented. By reviewing site-monitoring reports, IRBs have the opportunity to ask whether sponsors have provided any additional training needed.
Following the Protocol. IRBs should also ask whether the protocol was followed. In 2005, one of the top five violations CDRH found during inspections of clinical investigator facilities was “failure of the clinical investigator to follow the protocol or investigational plan” (see Table II). If a sponsor is monitoring the study, and if a sponsor's monitors are trained to find noncompliance, that violation should never occur. IRBs should also ask whether the protocol has been followed and report on it so the clinical investigator acquires additional training on the protocol.
Device Accountability. Asking about device accountability is also important, because the answers can alert IRBs to possible use of an unapproved device outside the study or alert them that the clinical investigator has more subjects in the study than are being reported.
Difficulty Using the Device. IRBs should also ask whether clinical investigators are having difficulty using the device. In one case, BIMO learned that an investigator was taking six hours to implant a device that should have taken about two hours to implant. That information was not submitted to the IRB, but it should have been because it was an unanticipated problem involving risks to the subject. In another case, the handle of an investigational device had to be broken to remove the investigational catheter. Such episodes may affect patient safety and the subject's willingness to continue participating in the study.
All unanticipated adverse device events or significant new information should be reported to IRBs, and IRBs should ask specific questions to elicit this type of information when they do their continuing review of the device study. FDA encourages IRBs to ask questions to elicit how the device study will be—or is being—conducted to better protect research subjects and ensure the quality of the study.
Ensuring an IRB Is Compliant. How do sponsors know whether IRBs are compliant with 21 CFR 56? Although this is not a stated requirement in the device regulations, it is a requirement of drug regulations (21 CFR 312), and it is recommended in ICH guidance documents.7–9 Sponsors can ask the clinical investigator to ensure that an IRB is functioning in compliance with the regulations. To ensure IRB approval of the study, sponsors should ask the clinical investigator for a copy of the IRB approval letter for the research. In FDA's view, this documentation provides the sponsor with reasonable assurance that an IRB complies with Part 56. Recently, some IRB approval letters have begun including a brief statement that the IRB is complying with Part 56. This appears to be becoming standard, and it may be in response to sponsors asking about IRB compliance with Part 56. Sponsors should also ask investigators to provide them with a copy of the IRB's continuing review letter and confirm that the IRB is performing continuing reviews during their site-monitoring visits.
Sponsors may also assess an IRB's compliance with FDA regulations by requesting its latest FDA Establishment Inspection Report. Although it is a snapshot in time, the latest report contains the most current and detailed information available. Sponsors may also check FDA's Web site for warning letters for the IRB. Bear in mind that FDA may not have inspected an IRB yet, so sponsors may want to audit the IRB and take a measured approach to ensuring the IRB's compliance.
Ensuring a Proper Informed-Consent Process. Besides ensuring that IRB approval is received before a study begins, ensuring that the consent process is handled properly is one of the most important things a sponsor can do.
Both 21 CFR 50 and 21 CFR 56 follow the principles in The Belmont Report.4,10,11 However, FDA receives complaints each year from research subjects who report that one or more of the requirements were not followed. In one case, a clinical investigator performed a study requiring an arteriogram without first obtaining consent. After a patient had agreed to enroll, the study coordinator had to find the patient's spouse in the waiting room to sign the informed consent, because at that point, the subject was already sedated. That is not the informed-consent process described in the regulations at 21 CFR 50, which requires the consent process to minimize undue influence, provide subjects with sufficient opportunity to consider their participation, and allow adequate time to read the document before it is signed and dated.
IRBs, clinical investigators, and sponsors should all respect the autonomy of each individual. Clinical investigators should solicit voluntary consent from informed subjects. That means that there can be no undue influence during the process or in the document itself. The consenting process and the document cannot promote the safety or effectiveness of the device, because that has not yet been proven. Subjects must understand that the research device is not FDA approved, nor approved for use in the United States.
Even though sponsors are not present during the informed-consent process, IRBs, sponsors, and clinical investigators should ensure proper solicitation of subjects. They can achieve this by doing the following:
• Providing all subjects time to consider their participation.
• Ensuring that each patient understands the explanations and language in the document (e.g., by using eighth-grade-level vocabulary in the text or by reading the consent form to patients).
• Including no language that waives the subject's legal rights or releases the sponsor or institution for negligence.
• Giving the subject adequate opportunity to read informed-consent forms before signing and dating them.
The informed-consent form must contain all of the required elements in 21 CFR 50 before it is sent to the IRBs for approval. Sponsors can also train clinical investigators in the informed-consent process and follow up during monitoring visits to ensure that the process has met FDA requirements. They can ensure that the most recent version of the informed-consent document was used to obtain the consent of each patient, and that patients are informed as new information becomes available that may affect their willingness to continue in the study. When using a contract research organization (CRO) to monitor a trial, it is important to read the monitoring reports and follow up rapidly with the CRO regarding any questions or concerns.
Even though sponsors, clinical investigators, and IRBs share responsibility for ensuring that subjects sign and date informed-consent documents before being enrolled in FDA-regulated research, FDA still finds that some subjects in the study do not sign and date the consent document. Although it is rare to find an entire study where the informed-consent document was not signed and dated, FDA more frequently finds that a few subjects in a study have not signed and dated the consent form. Bear in mind that FDA does not require a clinical investigator to sign the informed-consent document, but the protocol, the IRB, or the sponsor may require it.
Conclusion
Ensuring that human subjects are protected is paramount to clinical studies. A strong sponsor-IRB relationship can improve the quality of device research. FDA encourages sponsors to develop effective approaches to better protect human subjects in device clinical trials.
However, a successful clinical trial does not end with protecting subjects. Future articles will discuss how to conduct device clinical trials and how to modify an existing quality system to the management of device clinical trials.
Acknowledgments
This article is based on a three-hour electronic conference presented on November 22, 2005, by members of FDA's Division of Bioresearch Monitoring, Office of Compliance, CDRH. The electronic conference was cosponsored by the Clinical Device Group, a consulting firm specializing in medical device premarket issues; and FDLI, a nonprofit organization providing education for the discussion of law and public policy issues. Special thanks go to Nancy Stark, PhD, president of Clinical Device Group (Chicago), for providing a CD of the conference for use in preparing this article. The CD is available for purchase from Clinical Device Group at www.clinicaldevice.com.
The contents of this article are the authors' views, and they do not necessarily reflect the views and policies of FDA or its staff. FDA will not be bound by any of the comments or information contained in this article.
Michael E. Marcarelli, Marian J. Serge, Jean Toth-Allen, and Cynthia A. Harris work in CDRH's Division of Bioresearch Monitoring. Barbara K. Immel is president of Immel Resources LLC (Petaluma, CA).
References
1. Michael E Marcarelli et al., “Integrating Quality into Device Clinical Trials” (presented at an e-conference, sponsored by Clinical Device Group and FDLI, November 22, 2005).
2. “FY 2006 Budget Summary and Budget in Brief” [online] (Rockville, MD: FDA: Field Activities—Office of Regulatory Affairs); available from Internet: www.fda.gov/oc/oms/ofm/budget/2006/PDFs/Summary/Pages300thru335.pdf.
3. “FY 2007 Budget” [online] (Rockville, MD: FDA: Field Activities—Office of Regulatory Affairs); available from Internet: www.fda.gov/oc/oms/ofm/budget/2007/HTML/7FieldActivitiesORA.htm.
4. Code of Federal Regulations, 21 CFR 56.
5. “Sponsor-Investigator-IRB Interrelationship, Information Sheets, Guidance for Institutional Review Boards and Clinical Investigators (1998 Update)” [online] (Rockville, MD: FDA); available from Internet: www.fda.gov/oc/ohrt/irbs/toc4.html.
6. Code of Federal Regulations, 21 CFR Part 812.
7. Code of Federal Regulations, 21 CFR Part 312.
8. “Guidance for Industry: ICH E6, Good Clinical Practice: Consolidated Guidance” [online] (Rockville, MD: FDA, 1996); available from Internet: www.fda.gov/cder/guidance/959fnl.pdf.
9. “ICH Harmonized Tripartite Guideline, Guideline for Good Clinical Practice, E6 (R1)” [online] (Geneva: International Conference of Harmonization); available from Internet: www.ich.org/LOB/media/MEDIA482.pdf.
10. Code of Federal Regulations, 21 CFR Part 50.
11. “The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research” [online] (Bethesda, MD: The National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research, 1979); available from Internet: www.fda.gov/oc/ihrt/irbs/belmont.html.
Copyright ©2006 Medical Device & Diagnostic Industry
About the Author(s)
You May Also Like


