Sign up for the QMED & MD+DI Daily newsletter.
Bob Michaels
March 6, 2014
5 Min Read
.svg?width=850&auto=webp&quality=95&format=jpg&disable=upscale "New Dimension to 3-D Printing: Modeling Aneurysms")
Hear Ankur Chandra present "Case study: Highly Accurate Prototyping for Medical 3-D Printing" at BIOMEDevice Boston, Wednesday, March 26 at 2:40 p.m. |
Virtually everyone today knows that 3-D printing can be used to create everything from prototypes, tools, and handguns to such synthetic organs and body parts as livers and ears. But less well known is that the technology is also a prime candidate for modeling diseases. For example, at the University of Rochester (Rochester, NY), researchers are using 3-D printing to model aortic aneurysms--bulges in the aorta that often result in death.
Patient-Specific Modeling
The advent of 3-D printing represents an entirely new way of modeling aneurysms, according to Ankur Chandra, associate professor of surgery and biomedical engineering at the University of Rochester, program director of the university's vascular surgery clinical residency program, and a practicing vascular surgeon.
|
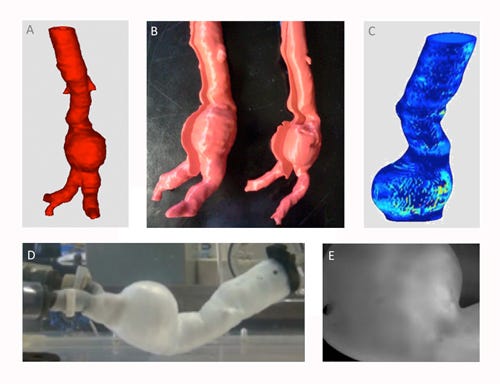
The five images above show the steps involved in creating and testing a 3-D-printed model of an abdominal aortic aneurysm: A. a 3-D reconstruction of a patient-specific aneurysm in .stl format generated using Mimics software; B. an ABS model of the inner and outer lumens of the aneurysm created using 3-D printing; C. a Matlab-generated heat map of the aneurysm undergoing wall strain; D. a PVA cryogel phantom of the aneurysm mounted and pressurized on a hemodynamic simulator; E. a high-speed video of the initial fracture and rupture point of the aneurysm during testing. |
"Based on patient CT data, we start by creating a patient-specific 3-D model of an aneurysm using Mimics and 3-matic software from Materialise NV (Leuven, Belgium)," Chandra explains. "Next, we print it using a biologically accurate material that simulates the properties of the aortic wall, and then we mount it on a hemodynamic simulator, subjecting it to such tightly controlled hemodynamic parameters as intraluminal pressures, blood flows, and cardiac outputs." As different hemodynamic and material properties change and stable aneurysms begin to fail, the researchers can study aneurysm behavior.
The development of aneurysms involves a very complicated interplay between environmental and genetic factors, according to Chandra. Exposure to tobacco smoke or other environmental factors, chronic hypertension, and biochemical changes in the aortic wall can combine to create a human-specific disease. Thus, aortic aneurysms have been very difficult to study both clinically and experimentally.
"To investigate most disease processes, you need a good animal model and the ability to study it experimentally," Chandra explains. "But because animals rarely develop aneurysms, most such studies involve infusing the aorta with a toxic substance or other material to degrade or inflame the wall, causing it to weaken. While this approach may work in certain studies on biochemical pathways, it cannot help to explain how overall biomechanical forces influence the degeneration and rupture of an aneurysm."
By the same token, using human models to study aneurysms is ethically fraught. "The ultimate outcome of aneurysms that we want to avoid is rupture, Chandra notes. "Because the rupture event is often fatal, we have not been able to conduct ethical human trials to the point of rupture to try to get an idea of what factors can predict these events." By foregoing the use of both animal and human models, such 3-D printing software suites as Mimics represent a genuine breakthrough in modeling aneurysm disease.
Vascular Device Design and Testing
Today, the development of most aortic medical devices, including aortic stents, is based on middle-of-the bell-curve models. Such models are used to determine the distances between certain branch vessels and the sizes of aortas and aneurysms. To create such devices, researchers rely on animal testing, at least at the beginning design stages. For example, device safety, fatigue, and failure modes are tested in animals.
"In contrast, with the ability to 3-D print aortic pathology, we will eventually be able to test many aortic devices in an ex vivo environment," Chandra says. "By implanting them into anatomy and physiology similar to those of humans suffering from aneurysms, we will be able to observe how these devices behave." Thus, medical device design, including in the vascular medicine space, is a potentially exciting 3-D printing application.
For example, 3-D printing could eventually enable medical device designers to design and model such complex vascular technologies as those used for performing aortic dissections, Chandra comments. "As we develop technologies for aortic dissection--a procedure that is very difficult if not impossible to reproduce in animals--and as we increase our ability to 3-D print actual dissections and then subject them to physiological pressures, we will learn how devices change the hemodynamics within the aorta and be able to observe some of the pressure distributions on the aortic wall."
Moreover, as complicated branched and fenestrated stents for treating different portions of the aorta are developed, 3-D technology could also enable researchers to study how the cardiac cycle and the motion of the aorta affect medical device materials and contribute to device fatigue. "One of the benefits of being able to 3-D print patients' anatomies and mount them on a simulator is that we can implant stents into physiologically accurate structures and cycle them for days, weeks, or months to observe how they behave," Chandra says. "As a result, we will be able to develop improved designs based on a more accurate testing platform."
While the efforts to develop a patient-specific vascular modeling platform based on 3-D printing technology are still a work in progress, the University of Rochester researchers have begun to partner with industry, pointing the way to the technology's eventual commercialization. The researchers also hope that 3-D printing will become part of the standard for device testing within the next few years.
"Aneurysms, Chandra comments, "are a low-prevalence, high-mortality disease. While they don't affect huge patient populations, as do hypertension and diabetes, the mortality rate associated with the untreated disease is very high. It therefore falls into the category of a disease in which risk prediction and screening are crucial. Not everyone has it, but for those that do, we need to figure it out."
Bob Michaels is senior technical editor at UBM Canon.
About the Author(s)
You May Also Like


